
Imagine taking a bite of your favorite meal, only to feel it get stuck halfway down. You swallow hard, maybe take a sip of water, but that heavy, uncomfortable sensation remains. For millions of people, this isn't just an occasional hiccup-it's a daily reality known as dysphagia. While many assume this is simply part of aging or a sign of acid reflux, it often points to a deeper issue: esophageal motility disorders, which are conditions where the muscles in your esophagus fail to coordinate properly, preventing food from moving smoothly into your stomach.
If you’ve been told you have "GERD" but proton pump inhibitors aren’t helping, or if you’ve experienced unexplained chest pain that mimics heart attacks, you might be dealing with one of these disorders. The good news? We now have precise tools to diagnose them. Let’s break down what these disorders are, how doctors spot them using advanced technology like manometry, and what treatment options actually work.
What Are Esophageal Motility Disorders?
Your esophagus is more than just a passive tube; it’s a muscular highway that uses rhythmic contractions called peristalsis to push food toward your stomach. At the bottom of this highway sits the lower esophageal sphincter (LES), a valve that opens to let food in and closes to keep stomach acid out. In healthy individuals, this process is seamless and unconscious.
In esophageal motility disorders, this coordination breaks down. The muscles may contract too weakly, too strongly, or at the wrong time. The LES might fail to relax when you swallow, creating a bottleneck, or it might stay open too much, causing severe reflux. These issues are classified into two main groups:
- Primary Motility Disorders: Problems intrinsic to the esophagus itself, such as achalasia, a condition where the esophagus loses nerve cells needed for relaxation, diffuse esophageal spasm, or jackhammer esophagus.
- Secondary Motility Disorders: Issues caused by systemic diseases affecting other parts of the body, most commonly systemic sclerosis (also known as scleroderma), which causes fibrosis and weakening of the esophageal muscles.
Achalasia is perhaps the most well-known primary disorder. It affects roughly 1 in 100,000 people annually. In achalasia, the LES doesn’t relax, and the esophagus above it stops contracting. Food pools up, leading to significant weight loss and regurgitation. Other types include "jackhammer esophagus," where contractions are excessively strong (pressures exceeding 5000 mmHg•s•cm), causing intense chest pain.
The Role of High-Resolution Manometry
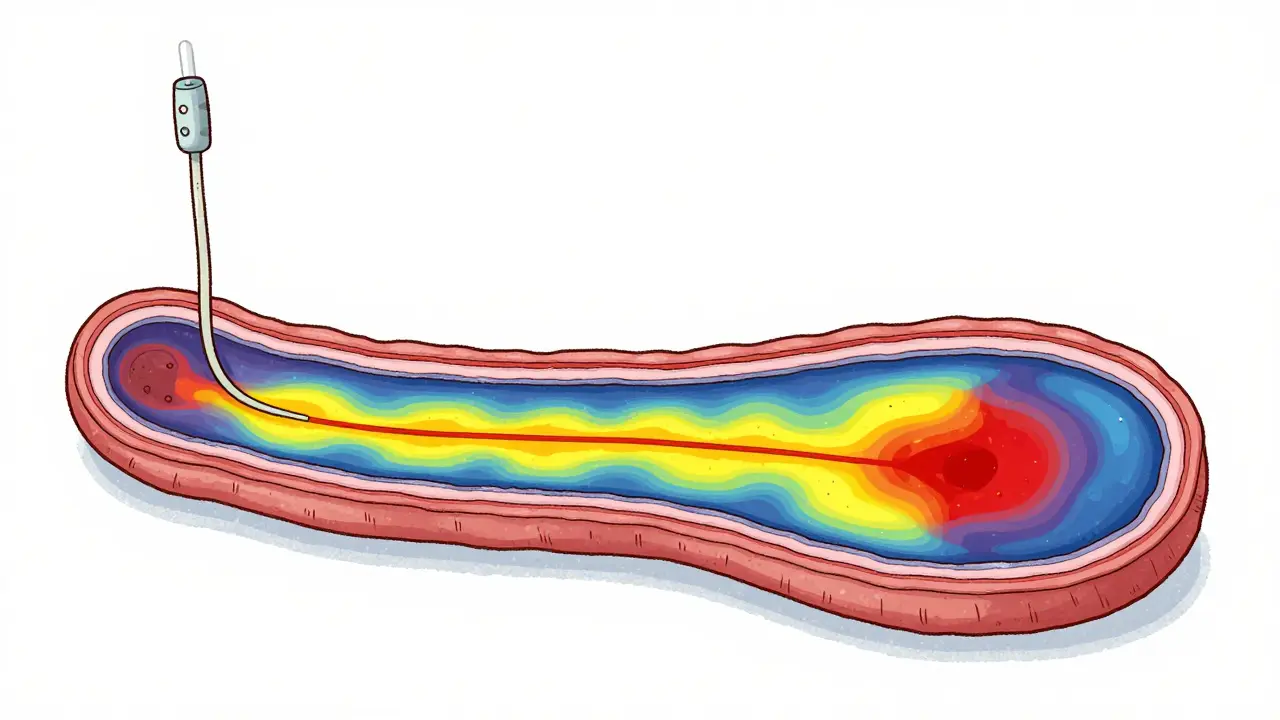
For decades, diagnosing these subtle muscle problems was like trying to read a book in the dark. Doctors relied on barium swallows, which show structural blockages but miss functional issues. Today, the gold standard is high-resolution manometry (HRM), a test that maps pressure changes along the entire length of the esophagus with incredible precision.
During HRM, a thin catheter with 36 circumferential pressure sensors is passed through your nose into your esophagus. As you swallow, these sensors create a color-coded topographic map of muscle activity. This allows gastroenterologists to see exactly where the coordination fails. Is the LES failing to open? Are there spasms in the middle of the esophagus? HRM provides the answers.
| Method | What It Measures | Sensitivity for Achalasia | Best Used For |
|---|---|---|---|
| High-Resolution Manometry | Muscle pressure and coordination | 96% | Diagnosing specific motility patterns (e.g., achalasia, spasm) |
| Barium Swallow | Structural anatomy and flow | 78% | Ruling out strictures or tumors |
| EndoFLIP (Impedance Planimetry) | Cross-sectional area and distensibility | 92% | Assessing EGJ outflow obstruction during dilation |
Why is HRM so much better? A 2020 study in *Diseases of the Esophagus* found that HRM has a 96% sensitivity rate for diagnosing achalasia, compared to just 78% for traditional barium studies. More importantly, HRM allows doctors to classify the disorder accurately, which dictates treatment. Not all motility issues are treated the same way.
Understanding the Chicago Classification v4.0
Data from manometry tests can look chaotic to the untrained eye. To bring order to this complexity, experts developed the Chicago Classification, a standardized system for interpreting manometry results. The latest version, v4.0, was published in 2023. It divides disorders into "major" categories that require treatment and "minor" variations that might be normal.
This classification system has dramatically improved diagnostic accuracy. Before v4.0, different doctors might interpret the same test differently. Now, inter-observer agreement has jumped from a moderate kappa value of 0.45 to an excellent 0.85. Here’s how the major disorders are categorized under v4.0:
- Achalasia Type I: Classic form with no peristalsis and incomplete LES relaxation (about 20% of cases).
- Achalasia Type II: Features pan-esophageal pressurization (pressure builds up throughout the esophagus). This is the most common type (70%) and responds best to treatment.
- Achalasia Type III: Spastic contractions occur before food reaches the LES (10% of cases).
- Jackhammer Esophagus: Hypertensive peristalsis with extremely high contraction strength.
- Diffuse Esophageal Spasm (DES): Premature, uncoordinated contractions causing chest pain and dysphagia.
The v4.0 update also introduced EGJ Outflow Obstruction (EGJOO) as a distinct entity. This occurs when the LES doesn’t relax fully, but peristalsis is still present. It’s a gray area that requires careful clinical correlation because not everyone with EGJOO has symptoms.
Treatment Options: From Medication to Surgery
Treating esophageal motility disorders depends entirely on the specific diagnosis. There is no one-size-fits-all pill. However, several effective interventions exist.
For Achalasia: Since the problem is mechanical (the valve won’t open), medication rarely works long-term. The two leading treatments are surgical:
- Laparoscopic Heller Myotomy (LHM): A surgeon cuts the muscle fibers of the LES to allow it to open. Often combined with a partial fundoplication to prevent reflux. Success rates are 85-90% at five years.
- Peroral Endoscopic Myotomy (POEM): A less invasive procedure where an endoscope is used to cut the muscle from inside the esophagus. POEM is equally effective as LHM but carries a higher risk of post-procedure reflux (44% vs. 29%).
For Spastic Disorders (Jackhammer/DES): Treatment focuses on relaxing the muscles. This starts with medications like calcium channel blockers or nitrates. If those fail, botox injections can be delivered directly into the esophageal muscle via endoscopy. In severe, refractory cases, surgery may be considered, though it’s less straightforward than for achalasia.
For Secondary Disorders: If scleroderma is the cause, treatment involves managing the underlying autoimmune disease and aggressively treating reflux with PPIs, since the LES is often too loose rather than too tight.
Why Diagnosis Takes So Long
One of the biggest frustrations for patients is the delay in getting answers. A survey by the International Foundation for Gastrointestinal Disorders found that 68% of patients waited 2-5 years for a correct diagnosis. Why? Because symptoms overlap significantly with GERD.
Many patients are misdiagnosed with acid reflux and prescribed proton pump inhibitors (PPIs) for years. Dr. Kristle Lee Lynch from the University of Pennsylvania notes that this leads to inappropriate treatment that doesn’t address the root motility problem. Chest pain from diffuse esophageal spasm is frequently mistaken for cardiac pain, leading to multiple emergency room visits.
To speed up your own journey, keep a symptom diary. Note whether solids or liquids are harder to swallow. Achalasia typically affects both equally, while structural blockages affect solids first. Mention chest pain explicitly to your doctor. If endoscopy shows a normal-looking esophagus but you still have trouble swallowing, ask specifically about motility testing.
Future Directions and Technology
The field is evolving rapidly. New technologies are making diagnosis easier and more comfortable. Wireless motility capsules (like the SmartPill) allow for ambulatory monitoring over 24-48 hours, giving a broader picture of esophageal function without a nasal catheter. Additionally, AI-assisted interpretation tools are being developed to help doctors read manometry charts with greater accuracy, potentially reducing diagnostic errors.
As awareness grows, more gastroenterology fellowships are incorporating formal motility training. The goal is to ensure that every patient with unexplained dysphagia gets the right test-the right answer-and ultimately, relief.
What is the difference between dysphagia and globus sensation?
Dysphagia is difficulty swallowing food or liquid, often due to a physical or motility blockage. Globus sensation is the feeling of a lump in the throat without actual difficulty swallowing. Globus is often related to anxiety or mild reflux, while dysphagia requires medical evaluation for motility disorders or structural issues.
Is high-resolution manometry painful?
Most patients describe it as uncomfortable but not painful. The catheter passes through the nose, which can cause some irritation. Numbing spray is used to minimize discomfort. The procedure takes about 30-45 minutes. About 35% of patients report significant discomfort, but satisfaction rises to 78% when they are properly educated beforehand.
Can esophageal motility disorders be cured?
While there is no cure for the underlying nerve or muscle dysfunction, symptoms can be effectively managed. Procedures like POEM or Heller myotomy can restore the ability to eat normally for many achalasia patients. Spastic disorders may require ongoing medication management.
What foods should I avoid if I have a motility disorder?
Avoid tough meats, dry bread, and sticky foods like peanut butter that are hard to swallow. Eat slowly, chew thoroughly, and drink water with meals to help move food through. Avoid very hot or very cold foods if they trigger spasms. Individual triggers vary, so keeping a food diary is helpful.
How does the Chicago Classification v4.0 change diagnosis?
Version 4.0 provides stricter criteria for diagnosing major disorders like achalasia and jackhammer esophagus, reducing false positives. It introduces EGJ Outflow Obstruction as a separate category, allowing doctors to distinguish between true motility failures and minor variants that may not need aggressive treatment.
Brett Webster
June 15, 2026 AT 12:02I had no idea manometry was this precise. The part about the Chicago Classification v4.0 really clarifies why my previous tests were so confusing. It is good to know that inter-observer agreement has improved significantly.
Miranda River
June 17, 2026 AT 05:30typo alert: you said 'jackhammer' but i think its actually just your nerves acting up lol. also why do we need a catheter in our nose? sounds like medieval torture disguised as science. maybe try yoga instead of poking holes in yourself. 🙄
Lee Coates
June 18, 2026 AT 21:33another day another american medical bill for a tube down the nose :P. love how they charge us extra for 'advanced technology' while basic care falls apart. typical. at least the diagnosis is quick if you can afford the test.
Sherry Wheeler
June 19, 2026 AT 23:02This is such a beacon of hope for those of us who have been dismissed with 'it's just stress' for years! I felt validated reading about the delay in diagnosis. Thank you for shedding light on this invisible struggle. It gives me courage to push for the right tests now!
Brandon Brodsky
June 20, 2026 AT 12:51Sarcasm aside, the stats on achalasia type II responding best to treatment are interesting. But let's be real, most people here will never get an HRM because their doctor thinks it's all in their head. Classic drama.
shreya sinha
June 22, 2026 AT 12:27It is quite disturbing to see how the modern medical establishment continues to prioritize expensive technological interventions over holistic and natural healing methods which have been proven effective for centuries in traditional systems of medicine. The reliance on invasive procedures such as high-resolution manometry reflects a profound lack of understanding regarding the body's innate ability to self-regulate and heal without external interference from foreign objects inserted into the nasal passages or esophageal tract. Furthermore, the classification systems developed by Western experts often fail to account for the subtle energetic imbalances that truly underlie motility disorders, thereby leading to misdiagnosis and inappropriate treatment protocols that further disrupt the patient's natural rhythm. One must question the ethical implications of promoting such aggressive diagnostic pathways when simpler, non-invasive approaches could potentially alleviate symptoms without causing additional trauma to the individual. It is imperative that we reconsider our approach to healthcare and integrate more compassionate and less intrusive methods into standard practice.
Ganesh Honikol
June 22, 2026 AT 16:30I completely agree with the sentiment expressed above regarding the importance of comprehensive care, although I believe that modern diagnostics play a crucial role in identifying specific physiological issues that cannot be addressed through lifestyle changes alone. However, it is essential that patients are fully informed about the benefits and risks of each procedure, ensuring that they make decisions based on accurate information rather than fear or misinformation. The integration of both traditional wisdom and contemporary medical science can lead to better outcomes for individuals suffering from complex conditions like esophageal motility disorders. We should strive for a balanced approach that respects the patient's autonomy and well-being.
Callie Skipper
June 23, 2026 AT 23:33i mean honestly just eat slower and chew your food more. half these problems come from wolfing down dinner while scrolling tiktok. not trying to be harsh but common sense goes a long way before you need a camera in your throat
Emily Barnhill
June 24, 2026 AT 17:21While lifestyle changes are helpful, dismissing severe motility disorders as merely a result of eating too fast is incredibly insensitive and medically inaccurate. Many patients suffer from neurological damage or structural abnormalities that no amount of chewing can fix. Please show some empathy to those genuinely struggling with debilitating symptoms that impact their quality of life daily. It is not about convenience; it is about survival and dignity.
AnneKatherine Stiekes
June 25, 2026 AT 21:45peace out everyone lets just focus on finding what works for each person since bodies are unique. no need to fight over methods
Christina S.
June 26, 2026 AT 23:20The section on POEM vs Heller Myotomy was super helpful for understanding the trade-offs. I appreciate the clear breakdown of success rates and reflux risks. Makes it easier to discuss options with a specialist.