
Statin Risk Calculator for Hypothyroid Patients
Calculate your risk of statin-induced muscle problems based on your thyroid function and the statin you're considering. This tool is designed for patients with hypothyroidism managing cholesterol levels.
When you’re managing hypothyroidism and need to lower your cholesterol, statins can feel like a double-edged sword. On one hand, they cut your risk of heart attack and stroke. On the other, they can cause muscle pain, weakness, or worse-especially if your thyroid isn’t properly controlled. This isn’t just a theoretical concern. Real patients are ending up in the hospital with muscle breakdown so severe it damages their kidneys. The good news? Most of these cases are preventable.
Why Hypothyroidism Makes Statins Riskier
Your thyroid doesn’t just control your energy levels or weight. It’s deeply involved in how your muscles and liver process drugs. When thyroid hormone levels are low, your body slows down key metabolic pathways. One of the biggest problems? Your liver can’t break down statins as quickly. This means more of the drug builds up in your bloodstream, increasing the chance of muscle damage. Statins themselves also interfere with muscle health. They reduce levels of coenzyme Q10, a compound your muscles need to produce energy. In people with hypothyroidism, mitochondria-the powerhouses inside muscle cells-are already struggling. Add a statin on top, and the energy deficit gets worse. Studies show this combo can cut cellular energy production by up to 40% in skeletal muscle. The result? Muscle pain, cramps, and weakness that aren’t just annoying-they can be dangerous. The risk isn’t small. A 2019 study of over 12,000 people found that those with untreated hypothyroidism were more than four times as likely to develop statin-induced myopathy compared to people with normal thyroid function. Even mild thyroid dysfunction (TSH between 4.5 and 10) raised the risk by more than double.Not All Statins Are Created Equal
If you have hypothyroidism, the type of statin you take matters just as much as the dose. There are two main groups: lipophilic (fat-soluble) and hydrophilic (water-soluble). Lipophilic statins-like simvastatin, atorvastatin, and lovastatin-easily slip into muscle cells. That’s why they’re more likely to cause problems in people with thyroid issues. Simvastatin at 40 mg or higher carries the highest risk. One analysis showed that 12.7% of hypothyroid patients on high-dose simvastatin developed muscle symptoms, compared to just 2.1% of those with normal thyroid levels. Hydrophilic statins, like pravastatin and rosuvastatin, don’t penetrate muscle tissue as easily. That makes them safer. Pravastatin, for example, has a myopathy rate of only 1.3% in hypothyroid patients. Rosuvastatin at 10-20 mg daily is now recommended as the first choice for people with thyroid disease by the 2023 Endocrine Society guidelines. Here’s what the data says about risk by statin:| Statin | Type | Myopathy Risk in Hypothyroid Patients | Recommended Dose Range |
|---|---|---|---|
| Simvastatin | Lipophilic | 12.7% (at ≥40 mg) | Avoid ≥40 mg; not recommended |
| Atorvastatin | Lipophilic | 7.8% | 10-20 mg preferred |
| Pravastatin | Hydrophilic | 1.3% | 20-40 mg |
| Rosuvastatin | Hydrophilic | 1.4% | 10-20 mg |
Thyroid Levels Are the Key
The biggest mistake doctors and patients make is starting a statin while thyroid levels are still out of range. Many people assume that if they’re taking levothyroxine, they’re fine. But “fine” isn’t good enough. The goal isn’t just to get your TSH into the normal range-it’s to get it into the optimal range. Research shows that TSH levels above 4.0 mIU/L increase statin myopathy risk. The American Thyroid Association now recommends keeping TSH between 0.5 and 3.0 mIU/L for people on statins. If your TSH is 7.0 or higher, the risk-benefit ratio of statins starts to flip. One expert, Dr. Robert Rosenson, says statin therapy becomes questionable when TSH exceeds 7.0. A 2022 study found that treating hypothyroidism to target TSH levels before starting a statin reduced muscle problems by 78%. That’s not a small gain-it’s life-changing. One patient on Reddit described CK levels spiking to 8,400 U/L after starting atorvastatin while his TSH was 9.2. After adjusting his thyroid meds, his symptoms vanished in three weeks.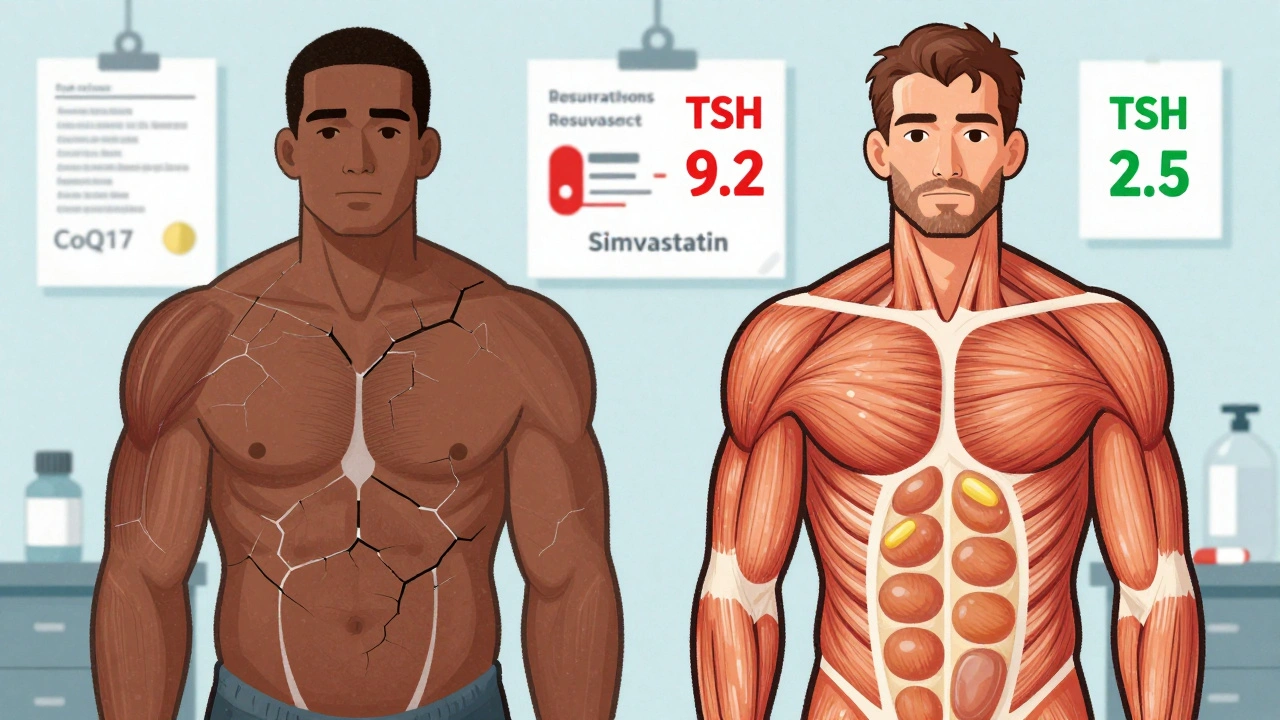
What to Do Before and After Starting a Statin
If you have hypothyroidism and your doctor wants to start you on a statin, here’s what you should ask for:- Get your TSH and free T4 tested before the first statin dose. Don’t assume your current dose is enough.
- Optimize your thyroid hormone first. If TSH is above 4.0, work with your endocrinologist to adjust your levothyroxine dose. Don’t rush-adjustments should be no more than 25 mcg every 4-6 weeks.
- Choose the safest statin. Ask for rosuvastatin or pravastatin. Avoid simvastatin entirely, especially at 40 mg or higher.
- Check your CK levels at baseline, then again at 3 months. If you develop muscle pain, cramps, or weakness, get tested immediately. CK levels above 5 times the upper limit of normal (ULN) with symptoms mean it’s time to stop the statin.
- Consider CoQ10. A 2020 trial showed 200 mg of CoQ10 daily reduced muscle pain by over 50% in hypothyroid patients on statins. It’s not officially recommended in all guidelines, but many doctors prescribe it off-label because it works.
What Happens If You Ignore This
This isn’t just about discomfort. Rhabdomyolysis-the breakdown of muscle tissue-is rare, but deadly. When muscle cells die, they spill a protein called myoglobin into the blood. Your kidneys can’t handle it. Acute kidney injury follows. The mortality rate for rhabdomyolysis with kidney failure is 10-20%. One case report from 2023 tells the story of a 67-year-old woman who developed CK levels of 28,500 U/L and needed dialysis. Her TSH? 22.4 mIU/L. She was on simvastatin 40 mg daily while preparing for radioactive iodine treatment. Her thyroid wasn’t being managed. Her statin wasn’t being adjusted. The result? A near-fatal event that could have been avoided with simple blood tests.
Why So Many People Stop Statins (And Why They Shouldn’t)
Here’s the heartbreaking part: 32% of hypothyroid patients stop their statins within a year because of muscle pain. That’s more than double the rate in people with normal thyroid function. But here’s the twist-most of those people could have kept taking them safely. A 2022 study found that 85-90% of hypothyroid patients who had their thyroid levels optimized were able to stay on statins without muscle problems. That means over 6 million Americans are unnecessarily skipping a medication that could prevent heart attacks and strokes. The economic cost? Statin-related hospitalizations cost $2,800 to $4,500 per episode. Rhabdomyolysis? Around $18,500. Preventing these events isn’t just about health-it’s about saving money.The Future: Personalized Risk Prediction
Science is catching up. A 2023 study in Nature Medicine identified a genetic risk score that combines thyroid-related genes and a gene called SLCO1B1-which affects how statins enter the liver. This score predicts myopathy risk with 82% accuracy. Imagine a blood test that tells you not just if you’re at risk, but which statin to take and at what dose. The European Medicines Agency is already moving to require warning labels on all statin packaging about hypothyroidism. The FDA is drafting similar guidance. And a clinical trial called THYROSIMVASTATIN, currently underway, will release results in early 2025. It’s testing a risk calculator that could one day tell your doctor: “For this patient, use rosuvastatin 10 mg, avoid simvastatin, and recheck TSH in 6 weeks.”Bottom Line: Control Thyroid, Keep Your Statin
You don’t have to choose between managing your thyroid and protecting your heart. The two go hand in hand. The problem isn’t statins-it’s uncontrolled hypothyroidism. If you’re on levothyroxine and your doctor wants to start a statin, say: “Let’s check my TSH first.” If your TSH is above 4.0, ask for a thyroid specialist consult. Don’t accept a statin prescription until your thyroid is in the sweet spot: 0.5-3.0 mIU/L. Pick rosuvastatin or pravastatin. Avoid simvastatin. Consider CoQ10. Monitor your muscles. This isn’t about fear. It’s about control. With the right steps, you can lower your cholesterol, protect your heart, and keep your muscles strong.Can hypothyroidism cause muscle pain even without statins?
Yes. Low thyroid hormone levels directly reduce muscle strength and energy production. Many people with untreated hypothyroidism report fatigue, stiffness, and cramps-even before starting any medication. These symptoms often improve once thyroid levels are corrected. However, when a statin is added, the muscle damage becomes more severe and can reach dangerous levels.
Should I stop my statin if I develop muscle pain?
Not necessarily. First, get your TSH and CK levels checked. If your TSH is high, adjusting your thyroid medication often resolves the pain without stopping the statin. If your CK is above 5 times the upper limit of normal and you have symptoms, your doctor may pause the statin temporarily. Many people can restart a different statin-like rosuvastatin-after their thyroid is optimized.
Is CoQ10 supplementation proven to help?
Yes, in clinical trials. A 2020 study showed that 200 mg of CoQ10 daily reduced statin-related muscle pain by 53.6% in people with hypothyroidism. While not yet officially recommended in all guidelines, many endocrinologists and cardiologists prescribe it because it’s safe and effective. It doesn’t replace thyroid treatment, but it can help bridge the gap while your levels stabilize.
Can I take a lower dose of statin to avoid side effects?
It depends. Lower doses of high-risk statins like simvastatin still carry elevated risk in hypothyroid patients. The better strategy is to switch to a safer statin like rosuvastatin or pravastatin at a low-to-moderate dose. These drugs are effective at lowering LDL even at low doses and have far fewer muscle-related side effects in thyroid patients.
How often should I get my thyroid checked while on statins?
Get your TSH tested before starting a statin, then again at 6-8 weeks after starting or changing the dose. After that, check every 6-12 months unless you’re adjusting your thyroid meds or experiencing muscle symptoms. If your dose changes, recheck in 6 weeks. Consistent monitoring is the key to staying safe.
Are there any natural alternatives to statins for hypothyroid patients?
Diet, exercise, and weight loss can help lower cholesterol, but they rarely bring LDL down enough for high-risk patients. Supplements like red yeast rice contain natural statins and carry the same muscle risks. Plant sterols and soluble fiber help a little, but they’re not substitutes for statins in people with a history of heart disease or high LDL. The safest path is optimizing thyroid function and choosing the right statin-not avoiding statins entirely.
Ollie Newland
December 5, 2025 AT 03:53Just had a patient last week with TSH at 8.3 on simvastatin 40mg. CK was through the roof. We switched to rosuvastatin 10mg, optimized levothyroxine, and added CoQ10. Three weeks later, he’s hiking again. This post nails it-thyroid first, statin second. No guesswork.
Rebecca Braatz
December 5, 2025 AT 06:27STOP letting doctors push simvastatin on hypothyroid patients. This isn’t just medical advice-it’s a lifesaving protocol. If your TSH is above 4, you’re playing Russian roulette with your muscles. Rosuvastatin isn’t ‘just another statin’-it’s the only safe choice. Share this with every thyroid group you’re in.
Michael Feldstein
December 6, 2025 AT 06:25Interesting breakdown. I’ve seen this play out in clinic too. The real issue isn’t the statin-it’s how we treat thyroid disease like a checkbox instead of a dynamic system. TSH 2.5 isn’t ‘normal,’ it’s ideal. And yeah, CoQ10 works. Not magic, but it’s the closest thing we’ve got to a buffer between statins and muscle pain. One patient said it felt like ‘turning a dimmer switch back on.’
jagdish kumar
December 8, 2025 AT 00:14Thyroid is the soul’s thermostat. Statins are the storm. When the soul is cold, the storm breaks bones.
Benjamin Sedler
December 9, 2025 AT 01:25So you’re telling me the entire medical establishment missed this for decades? That’s rich. Meanwhile, I’ve been taking grapefruit juice with my statin and drinking celery juice for ‘thyroid support.’ My CK levels are fine. Maybe the real problem is that doctors don’t listen to patients who aren’t wearing lab coats.
zac grant
December 10, 2025 AT 11:03Biggest takeaway: optimize TSH before statin initiation. Period. I’ve had patients come in with CK >10,000 because they were told ‘your thyroid is fine’ at TSH 6.8. Nope. Not fine. Not even close. Rosuvastatin 10mg + TSH 1.8 = zero muscle symptoms. The data is crystal clear. This isn’t anecdotal-it’s practice-changing.
michael booth
December 10, 2025 AT 20:37It is imperative that thyroid function be assessed prior to initiation of statin therapy in all patients with documented hypothyroidism. Failure to do so constitutes a preventable adverse event of significant clinical consequence. Rosuvastatin and pravastatin are preferred agents. Coenzyme Q10 supplementation demonstrates statistically significant reduction in myalgia. Monitoring CK at baseline and at three months is standard of care.
Carolyn Ford
December 12, 2025 AT 14:38Oh, so now we’re blaming hypothyroidism for statin side effects? Funny-I’ve been on levothyroxine for 12 years, TSH 1.9, and I still get muscle cramps on rosuvastatin. So what? Maybe it’s not the thyroid. Maybe it’s the statins. Maybe the whole ‘safe statin’ narrative is just pharma propaganda. You’re all too quick to blame the thyroid. What about your own biases?
Heidi Thomas
December 13, 2025 AT 17:14CoQ10 doesn’t work. I tried it. My muscles still hurt. This whole post is just fearmongering. Statins are dangerous. Period. Thyroid has nothing to do with it. You’re just trying to make people feel better about taking a toxic drug. I stopped mine and my cholesterol is fine. I eat kale and walk 10k steps. You can’t argue with results.
Rudy Van den Boogaert
December 15, 2025 AT 00:45Heard a great story from a cardiologist friend-patient on simvastatin 80mg, TSH 11, CK 30k. Got dialysis. After thyroid fix and switch to pravastatin 40mg? Back to golfing in 6 weeks. The scary part? This isn’t rare. It’s routine. Why aren’t we screening TSH before every statin script? Because it’s easier to write the prescription than to do the work.
Shofner Lehto
December 16, 2025 AT 05:27Just want to say thank you for this. My mom was on simvastatin for years, TSH was never checked. She ended up in the ER with rhabdo. We didn’t know any of this. This post is the exact info we needed six months too late. Please share this with your doctors. It’s not just about cholesterol-it’s about not ending up on dialysis.
Yasmine Hajar
December 16, 2025 AT 14:28As someone from a culture where thyroid issues are often dismissed as ‘just stress’ or ‘being lazy,’ this hits hard. In my community, people suffer for years before getting tested. And then they get statins without even knowing their TSH. This isn’t just medicine-it’s equity. We need to make this info accessible in Spanish, Hindi, Mandarin. No one should die because they didn’t know to ask for a TSH test before taking a statin.